
One method of understanding the workings of the black box brain is to observe what happens when it departs from normal baseline, desired behavior. For example, what can postpartum depression tell us about the brain? Do the treatments work and if so, what do those treatments also tell us about the brain? How do we diagnose or even define postpartum depression and what does that tell us about the brain?
Let us break it down and
start with depression. The
standard Diagnostic and Statistical Manual of Mental Disorders, edition 4
(DSM-IV) states that a unipolar, major depressive episode (i.e.
depression) exhibits itself in a severely depressed mood for at least 2
weeks. Starting from here, we
already have a complication. General
health practitioners have more discrete and objective diagnostic
guidelines: they diagnose strep throat for example not by observing a sore
throat lasting more than 2 weeks but rather by the presence of any
detectable streptococcal
bacteria in the throat. In
contrast, whether a patient is diagnosed as suffering from depression
depends on whether the patient expects to be depressed.
A person mourning or grieving is not depressed, though a person
mourning or grieving for too long or for no apparent loss is.
Hidden but implied in that diagnostic manual description is the
phrase, “abnormal, unexpected, and persistently depressed mood not
commensurate with recent experienced events in the patient’s primary
culture.” That is a lot of
subjective words.
Treatment depends on the diagnosis and causal model.
Since the starting diagnosis is already complicated, the treatment
issue becomes more difficult. Again,
general medicine has the objective advantage: if strep throat is caused by
the presence of streptococcal bacteria, eradicating the bacteria cures the
disease. Originally, the
causal model for any mental disorder – depression did not have its own
specific classification until fairly recently – included evil spirits.
Hundreds of years ago, treating depression did not so much involve
physicians as it did exorcists. By
about the 19th century with the industrial revolution in full
swing, the causal model shifted to include a focus on the imbalance of
environment. Treatment during this period involved removing the patient
from the chaotic environment causing the imbalance to a peaceful retreat
called a sanitorium. By about
the mid-20th century, the causal model shifted again with the
discovery of the first anti-depressants: tricyclics and monoamine oxidase
inhibitors (MAOIs). Oddly
enough, it was the discovery of the treatments that triggered the causal
model shift rather than the other way around.
A monoamine is a type of neurotransmitter that includes a
single (the “mono-“ prefix) amino acid (the “-amine” suffix).
A prime example is dopamine. Dopamine
is a feel-good transmitter and also involved in reward based learning.
This is the transmitter through which highly addicative and illegal
drugs such as cocaine work. Oxidization
is the breaking down process, so a monoamine oxidase (MAO) is a compound
that destroys monoamines, including dopamine.
Finally, an MAO inhibitor (MAOI) prevents the MAO from destroying
the dopamine, allowing the dopamine to continue acting as a feel-good
transmitter. Tricyclics and
later, more advanced selective serotonin reuptake inhibitors (SSRIs) work
under similar principles, but with slightly different targets. Discovering that these drugs can stop the compounds that
cause depression includes the discovery that some compounds can cause
depression.
But again, since the underlying diagnosis comes from a
subjective definition and not the presence of a foreign contaminant –
everyone has MAOs in their body, but only some have depression – the
practicing physician is forced to prescribe drugs and check if it stops
depression. If it did, then
the patient was depressed and now is not.
If it did not, then the patient was not depressed, at least not in
the way that can be treated with drugs.
The treatment confirms or pehaps even decides the diagnosis.
This is how the treatment triggered the causal model shift rather
than the other way around. Reversing
the normal order in this manner introduces many more risks because the
underlying causal model is less well understood.
The treatments are more likely to have unintended consequences.
The state of affairs with depression is messy and not at
all objective or clear cut. This
is a function not of our professional physician training but of the
incomplete model of the brain. While
this is fine to acknowledge in theory, what can be done in practice? We can do what any scientist would do: focus on a subset,
analyze the data, and form a model of the specific phenomenon that may
hopefully shed light on the phenomenon in general.
Postpartum depression is one such specific subset.
Postpartum depression affects 5-25% of all new mothers.
It can also affect new fathers.
Symptoms include, but are not limited to:
- Easily
frustrated
- Feeling
inadequate
- Low
self-esteem
- Social
withdrawal
- Sadness
- Guilt
- Overwhelmed
feeling
- Exhaustion
The first half of the symptoms suggest personality traits.
Someone easily frustrated faces more difficulties in performing
tasks, to the point where the cost of continuing to completion exceeds
available resources. Repeated incomplete tasks makes one feel inadequate and
withdrawn with low self-esteem. Being
isolated out of a sense of failure allows the constant refrain of failure
to echo in the thoughts, supporting a self-sustaining recurrent feedback
loop. The second half of the
symptoms would aptly describe the state of affairs at this point.
Placing this chain of events into a simplistic work flow in
parallel with the dopamine traces would look like this:
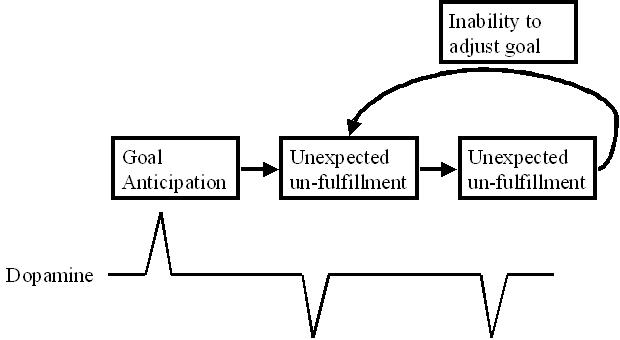
The dopaminergic reward based learning mechanism is well
documented – dopamine levels spike above baseline upon anticipation of a
reward, stay level on receipt of anticipated reward, and crash on
unexpected miss of a reward. Since
dopamine is a feel-good transmitter, the spikes feel good (e.g. evening
before an expected big birthday party with presents) and the crashes feel
bad (e.g. everyone forgot the birthday and no presents).
In terms of postpartum depression, the goal anticipation may be
that the new mother and father expect to be the best, ideal parents for
their child. The infant then
cries for food, cries for company, cries for entertainment, cries for
diaper changes, cries for exercise, and cries for the the sake of hearing
crying. The goal apparently
is missed since few parents expect ideal parenting to result in crying. But the final key is that infant calls are naturally pitched
to prevent parents and caregivers from adjusting their goals away from
being the best, ideal parents. Infant
cries are very difficult to ignore – perhaps it is evolution. But that results in a lot of dopamine crashes.
There is internal feedback – the sense of failure from
missing the goal due to infant crying increases doubt that increases the
cost of accomplishing tasks that slows down task accomplishment that
causes more missed goals. There
is external feedback – the infant is crying and constantly reminding the
parents of apparently missed goals.
An MAOI, for example, would remove those dopamine crashes
and extend those dopamine spikes. It
would reduce the bad feelings, reduce the doubt, reduce the cost of
accomplishing tasks, and allow the afflicted parent to function
effectively. But besides the
somewhat discomforting concept of a pill that removes doubt, the
dopaminergic reward based learning system requires dopamine spikes and
crashes to learn. Removing
this action implies it would impair learning.
Addressing postpartum depression within this dopamine
system entails adjustments through learning.
In the birthday party example, the subject learns that sometimes
people forget to organize large parties with many presents. The subject may need to remind others of the date.
Whether this is done directly or subtly depends on the culture and
the art form. Regarding
postpartum depression, perhaps this involves setting up the initial goal
before the infant’s birth to include crying as a part of life.
Or perhaps it involves enlisting support of some form such that the
parents feel comfortable enough to adjust their goals and directions in
the face of unknown doubts and very loud crying.
This may involve support groups or cognitive behavioral therapy.
The specifics are beyond the scope of this post as it may require
the input of many more experienced and knowledgable experts.
However, by understanding a different causal model of postpartum
depression, parents may be able to address potential issues by first
working with their brain and learning mechanisms while retaining the final
safety net of overriding them via anti-depressants only as necessary.