
In the movie, Eternal Sunshine of the Spotless Mind, depressed ex-lovers burdened by their emotional memories seek relief by having said memories surgically removed. The premise is theoretically possible. Strap on a neural monitor (e.g. fMRI, EEG), recall the pain-inducing memories, record which neurons were active, and surgically remove or lesion those targeted neurons. Et voila! Selective amnesia. The memory is either erased or at least the required neural machinery to recall them is missing. In computer-speak, the physical memory has been overwritten with zeros or the memory is de-referenced and not recallable.
It is theoretically possible, but this depends strongly on which theory. Unfortunately, there is not just one theory. As regards the surgical feasibility, there would be two major competing theoretical families: let us call them the encapsulated independent memory and the shared dependent memory.
In the first theory family, memories are stored distinctly and independently. The minimal neural architecture required to store one memory is one neuron. Say, the memory of the Ex-Lover is on neuron id #54354Yef-003, while the memory of the Best Friend is on neuron id #54354Yef-004. Place the patient in a brain scanner, monitor brain activity like a Predator drone, identify the proper coordinates at neuron id #54354Yef-003, and later drop a precision lesion agent to dissolve that neuron. The patient leaves outpatient surgery with no memory of the Ex-Lover, but fully able to retrieve the Car Keys to drive away with the Best Friend towards an upcoming Vacation. The operation is a success with no collateral damage. That is, if and only if the encapsulated independent memory theory is an appropriate one.
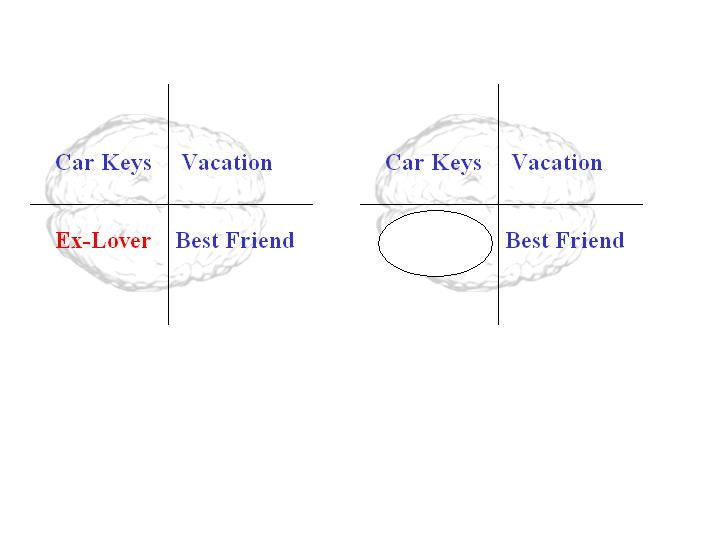
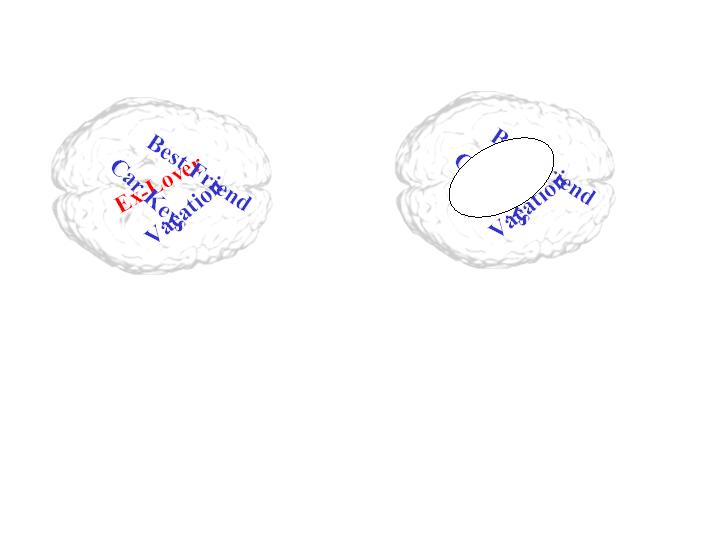
Under the alternative, shared dependent memory, all bets are off. Memories are interleaved and shared across the entire neural architecture. Every single neuron works together in a group dance to signify the Ex-Lover crossed with nearly everything else. Should we place the patient in a brain scanner, monitor brain activity like a Predator drone, identify neuron id #54354Yef-003 as lighting up strongly when thinking about the Ex-Lover, and later drop a precision lesion agent to dissolve that neuron, we would have successfully lobotomized the patient. The patient leaves outpatient surgery with no obvious memory of the Ex-Lover, but drools on a nice stranger who for some reason escorts them in a strange four-wheeled contraption towards an upcoming Vacation. The operation is a success, but with heavy collateral damage. And the Ex-Lover may still come to mind from time to time albeit less strongly in residual memories.
Debating which model family is more accurate or more appropriate is not the purpose here nor should it be. Simply put, there is a reason for the division in theory families. It is no more fruitful to debate the finer points of who is right and who is wrong than to debate Democrats vs. Republicans. It may be that both are correct in their particular fashion and scale of reference. It is not simply that the side effect is a risk under the second theory but not the first. Rather, it is that the side effect affects both theories, but the second more prominently highlights it.
But what do we do about the traumatic memory of the Ex-Lover that causes the patient to break down in tears? How do we make Jim Carrey’s character back to his lovable Mask - Pet Detective self? (Even if his performance, personally, was wonderful in Eternal Sunshine of the Spotless Mind.) Can he take a healthy, fat-free, surgery-free pill to forget his Ex-Lover?
There is another theory of memory consolidation (Squire & Alvarez, 1995) into long-term memory. The basic concept is as follows: experiences enter the brain’s hippocampus as short-term memory, ready to be wiped and forgotten unless they are consolidated into the brain’s cortical area as long-term memory. This process requires protein synthesis to operate. Certain compounds (e.g. anisomycin, Cohen, et al., 2006) can inhibit this process and allow the labile memory to pass into oblivion without consolidation into long-term memory. In computer-speak, the RAM memory file needs to be saved to the hard drive/flash drive/cloud before it is overwritten by other RAM files. Interfere by temporarily jamming the writing head effectively erases that memory file.
The catch is that this memory consolidation appears to occur both during initial memory experience and during later recall of the same memory. Interfere with its later re-consolidation and the effect is the same: erasure of the vulnerable memory. In computer-speak, the memory file is never copied, only cut-and-pasted.
The real catch is that this still makes no difference. Whether we have physically removed the underlying brain tissue that holds the memory or we have pharmacologically removed the overlying memory on that brain tissue still leaves us at the mercy of collateral damage. Never-mind the ethics or abuse of this potential memory erasure. The collateral damage ensues because memories may not be distinct, passive data objects for us to manipulate. Rather, they may be dynamic hierarchical elements that manipulate us. In computer-speak, that is… well, there is no such analog.
We may have fallen many times as infants learning to crawl and then to walk. It may have been traumatizing to fall over and over again. But if we remove the traumatic memories of crawling and falling, even without physically or logically impairing the memory of walking successfully, we may end up like our friendly ASIMO here. That is beautiful walking, as ASIMO was intended. But ASIMO has no memory of being able to crawl. That is why it cannot get up or continue.
A human memory is not like a computer memory. A human memory may be a mosaic, whereby each memory biases our decisions – including our decision to look in this direction or that direction and pay attention. These attention decisions dictate what we experience. These experiences form our memories. It is a great big feedback loop. Under this theory, removing a memory – irregardless of whether we have successfully spared the physical neuron or any other memory – still corrupts all other memories since the context has shifted. It is like a family photo with Mom, Dad, little Jimmy, and Uncle John. Erasing any single member ex post facto casts reverberating inexplicable inconsistencies on everyone else. All other memories start to make less sense. “Why did we go to ____’s house for vacation on the ____ days? That makes no sense! Maybe we didn’t really go there? Was that a dream?” “Maybe I am not such a loving family person after all?”
It matters not whether we have spared Jim Carrey’s character the drooling, lobotomized, crippling side effects in the quest to rid him of the traumatic memories. In this case, successfully removing the past memory is a failure in and of itself. Something must be done, but maybe imposing a computer architecture on our understanding of the brain is not an entirely helpful perspective.
The truth is, there is no clear answer here for dealing with the post traumatic stress of being burdened by emotional memories of, say, breaking up with an Ex-Lover. The body and the brain are far more messy than we would like. Maybe Jim Carrey’s character would be better served getting a new Lover. Maybe he would be better served writing a screenplay or poem or song about his Ex-Lover. Maybe he would be better going traveling to the jungles or on safari. And by so doing, honor his memory of the Ex-Lover by biasing and coloring in all future memories with his newly grown self.